set.seed(3672)
ng <- 250; g <- rep(0:1, each = ng); n <- 2 * ng
x <- rnorm(n); tau <- 0.6; beta <- 0.5
y_true <- 0 + tau * g + beta * x + rnorm(n, 0, 1)
## missing at random on x: higher x makes y more likely to be missing (about 35%)
aM <- uniroot(function(a) mean(plogis(a + x)) - 0.35, c(-6, 6))$root
my <- runif(n) < plogis(aM + x)
y <- y_true; y[my] <- NAChecking missing-data assumptions
R
missing data
simulation
ggplot2
Probing the missing-at-random assumption in R: a logistic missingness check, an observed-versus-imputed diagnostic, and a delta sensitivity analysis that finds the tipping point.
Every method in this series has leaned on one assumption: that the data are missing at random, so that what you observe is enough to stand in for what you do not. The awkward fact, established in the first post, is that this assumption cannot be tested against the recorded data. No diagnostic can separate missing at random from missing not at random, because the two differ only in how missingness relates to values you never see. So the honest response is not a test but a two-part discipline: check what can be checked, the imputation model, and then probe what cannot, the mechanism, by asking how wrong the assumption would have to be to change the answer. This closing post does both.
The example is a two-group comparison. A treatment is applied to half the sample, the outcome y has a true effect of 0.6, and y is missing at random given a covariate x.
About 31% of outcomes are missing, similar in both groups (32% and 30%). Multiple imputation under the working assumption, imputing y from group and x, recovers the effect:
m <- 40; nu_com <- n - 3
imps <- lapply(1:m, function(k) step(y, my, cbind(g, x)))
eff <- function(yc) { f <- lm(yc ~ g + x); c(coef(f)["g"], summary(f)$coef["g", 2]) }
E0 <- sapply(imps, eff)
p0 <- pool(E0[1, ], E0[2, ], m, nu_com); tcrit <- qt(0.975, p0["df"])
c(effect = unname(p0["Q"]),
lo = unname(p0["Q"] - tcrit * p0["se"]), hi = unname(p0["Q"] + tcrit * p0["se"])) effect lo hi
0.6392442 0.4241224 0.8543660 The pooled effect is 0.639, with a 95% interval of 0.424 to 0.854, comfortably clear of zero. Taken at face value, the treatment works. The rest of the post asks how much that conclusion depends on the assumption.
What the observed data can rule out
One thing the data can do is reject the strongest assumption, that the gaps are completely at random. If missingness is unrelated to everything observed, then a model predicting whether a value is missing from the observed variables should find nothing. Fit that model.
mcar <- glm(my ~ g + x, family = binomial)
round(summary(mcar)$coefficients, 3) Estimate Std. Error z value Pr(>|z|)
(Intercept) -1.021 0.158 -6.451 0.000
g -0.022 0.215 -0.101 0.919
x 1.118 0.130 8.587 0.000The coefficient on x is large and its p-value is effectively zero, so missingness depends strongly on the observed covariate: not missing completely at random. The coefficient on group is near zero (p 0.92), so the two groups drop out at similar rates. This is the formal ground for a missing-at-random analysis over a complete-case one, and it is what a test such as Little’s omnibus check (Little 1988) formalises across many variables at once. What it cannot do is go further. The same observed association with x is exactly what missing at random and missing not at random both predict; the test rejects complete randomness and then falls silent on the distinction that actually matters.
A diagnostic that checks the model, not the mechanism
The next instinct is to compare the values the imputation invents against the values that were seen, and worry if they differ. Figure 1 shows that comparison.
obs_y <- y[!my]; imp_y <- unlist(lapply(imps, function(v) v[my]))
df1 <- rbind(data.frame(y = obs_y, src = "Observed"),
data.frame(y = imp_y, src = "Imputed (pooled)"))
mu1 <- df1 |> group_by(src) |> summarise(m = mean(y), .groups = "drop")
ggplot(df1, aes(y, colour = src, fill = src)) +
geom_density(alpha = 0.16, linewidth = 0.8) +
geom_vline(data = mu1, aes(xintercept = m, colour = src),
linetype = "dashed", linewidth = 0.5, show.legend = FALSE) +
scale_colour_manual(values = c("Observed" = "#356170", "Imputed (pooled)" = "#c08a3e")) +
scale_fill_manual(values = c("Observed" = "#356170", "Imputed (pooled)" = "#c08a3e")) +
labs(title = "Observed against imputed: a model check, not a mechanism test",
subtitle = "A gap between the two is expected under missing at random",
x = "Outcome y", y = "Density", colour = NULL, fill = NULL) + theme_te()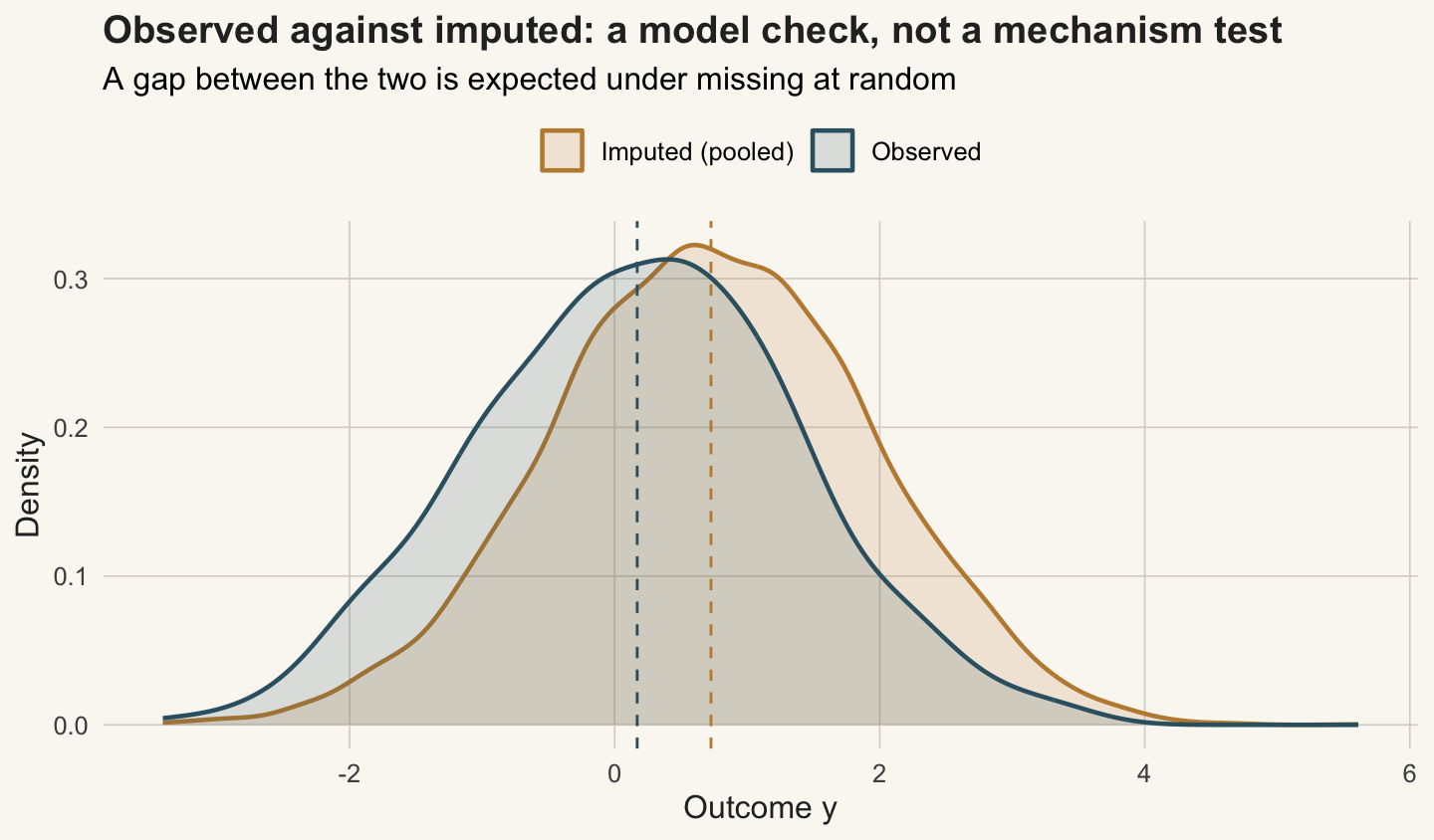
The imputed outcomes sit a little below the observed ones. It is tempting to read that as a problem, but it is not: the missing rows are the high-x rows, and higher x means a lower y, so an imputation that is working should place them lower. A diagnostic like this earns its keep by catching imputations that are plainly wrong, values outside the possible range, a bimodal shape where the data are unimodal, impossible negative counts. It confirms the imputation model is behaving. It says nothing about whether the mechanism is missing at random, because both mechanisms are consistent with this picture.
Probing the mechanism with a delta shift
If the assumption cannot be tested, the remaining move is to break it deliberately and watch. Suppose the outcomes are missing not at random in the worst plausible way: the people in the treatment group who dropped out did so because they were doing badly, so their true outcomes are lower than a missing-at-random imputation assumes, by some amount delta. Shift every imputed treatment-group outcome down by delta, re-pool, and sweep delta across a range. This is a pattern-mixture, or delta-adjustment, sensitivity analysis.
deltas <- seq(0, 1.5, 0.025)
trtmiss <- my & (g == 1)
sweep <- t(sapply(deltas, function(dl) {
ests <- ses <- numeric(m)
for (k in 1:m) { yc <- imps[[k]]; yc[trtmiss] <- yc[trtmiss] - dl
e <- eff(yc); ests[k] <- e[1]; ses[k] <- e[2] }
p <- pool(ests, ses, m, nu_com); tc <- qt(0.975, p["df"])
c(delta = dl, est = p["Q"], lo = p["Q"] - tc * p["se"], hi = p["Q"] + tc * p["se"])
}))
sweep <- as.data.frame(sweep); colnames(sweep) <- c("delta", "est", "lo", "hi")
tip <- sweep$delta[which(sweep$lo <= 0)[1]]
c(mar_effect = round(sweep$est[1], 3), tipping_delta = round(tip, 3)) mar_effect tipping_delta
0.639 1.350 At delta zero (missing at random) the effect is 0.639. As the assumed shortfall grows, the effect shrinks steadily: 0.485 at half a standard deviation, 0.331 at a full one. The interval first touches zero at a delta of 1.35. Figure 2 traces the whole path.
ggplot(sweep, aes(delta, est)) +
geom_ribbon(aes(ymin = lo, ymax = hi), fill = "#4a7a8c", alpha = 0.18) +
geom_line(colour = "#356170", linewidth = 0.9) +
geom_hline(yintercept = 0, colour = "#a24b4b", linetype = "dashed", linewidth = 0.6) +
geom_vline(xintercept = tip, colour = ink, linetype = "dotted", linewidth = 0.6) +
annotate("point", x = 0, y = sweep$est[1], colour = ink, size = 2.6) +
annotate("text", x = 0.03, y = sweep$est[1] + 0.06, label = "MAR (delta = 0)",
hjust = 0, size = 3.3, colour = ink) +
annotate("text", x = tip, y = 0.7, label = sprintf("tipping point\ndelta = %.2f", tip),
hjust = 1.08, size = 3.3, colour = ink, fontface = "bold") +
labs(title = "How far from MAR before the effect disappears",
subtitle = "Red line: no effect. The conclusion holds until the departure exceeds the tipping point",
x = "Delta: assumed shortfall of treatment dropouts (outcome SD units)",
y = "Estimated treatment effect") + theme_te()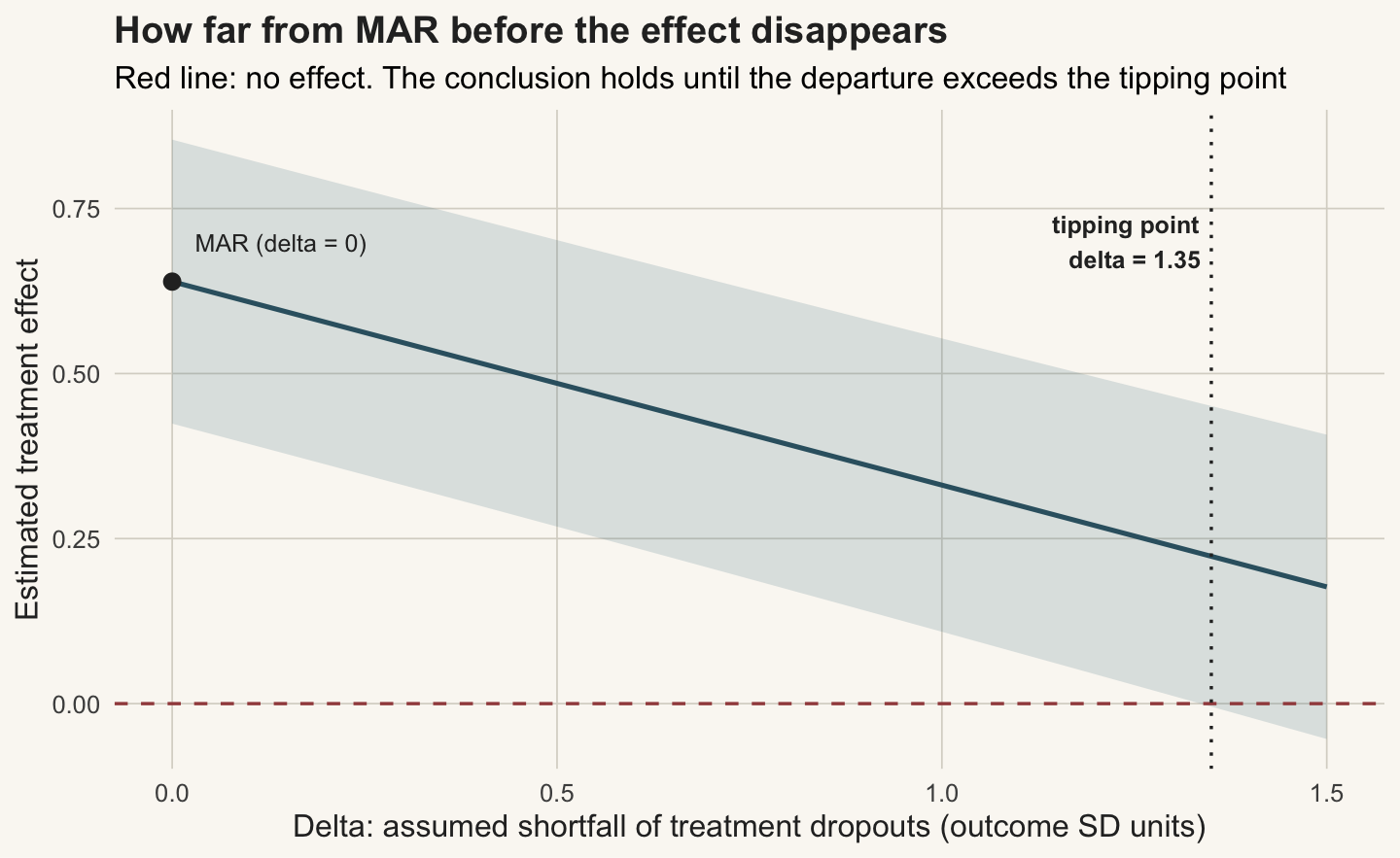
The honest limit
The tipping point is the whole point. The data cannot tell you the true delta, so a sensitivity analysis does not resolve the question; it relocates it. Instead of an untestable yes-or-no about missing at random, you are left with a quantity you can reason about: the treatment effect survives unless the dropouts in the treatment arm were doing worse than a missing-at-random imputation assumes by more than 1.35 standard deviations of the outcome. That is a large and specific departure, and whether it is plausible is a question for what is known about the study and its dropouts, not for the dataset. A small tipping point would be a warning that the conclusion rests on the assumption; a large one, as here, is reassurance that it does not rest on it much.
This is the same move that closes the measurement-error and causal-inference threads on this blog. None of them makes an untestable assumption testable. What they do is convert it into a magnitude, quantify how large a violation the conclusion could absorb, and hand that number back to the reader to judge. For missing data specifically: check the model with diagnostics, reject complete randomness where you can, and then report the tipping point rather than a bare interval that hides the assumption it depends on. If a real decision turns on the result, the delta you are willing to defend is part of the analysis, not an afterthought.
References
Rubin DB 1976. Biometrika 63(3):581-592 (10.1093/biomet/63.3.581).
Little RJA 1988. Journal of the American Statistical Association 83(404):1198-1202 (10.1080/01621459.1988.10478722).
Little RJA 1993. Journal of the American Statistical Association 88(421):125-134.
van Buuren S 2018. Flexible Imputation of Missing Data, 2nd edn. Chapman and Hall/CRC (10.1201/9780429492259).
Carpenter JR, Kenward MG 2013. Multiple Imputation and its Application. Wiley. ISBN 978-0-470-74052-1.
Molenberghs G, Kenward MG 2007. Missing Data in Clinical Studies. Wiley. ISBN 978-0-470-84981-1.
National Research Council 2010. The Prevention and Treatment of Missing Data in Clinical Trials. National Academies Press. ISBN 978-0-309-15814-5.
Johnson TF, Isaac NJB, Paviolo A, Gonzalez-Suarez M 2021. Global Ecology and Biogeography 30(1):51-62 (10.1111/geb.13185).